AI-Powered Compliance Platform for Life Sciences
April 24, 2026

A unified PSP data layer is a centralized integration architecture that consolidates patient, service, and outcome data from all patient support program vendors into a single, governed environment — without replacing the vendors themselves. It connects existing vendor systems through standardized APIs (FHIR, HL7), a common data model, a master patient index, and a shared audit log layer, giving pharmaceutical manufacturers a single source of truth across enrollment, benefits verification, adherence tracking, call centre operations, and pharmacovigilance reporting.
The problem it solves is structural: most pharmaceutical companies run PSPs through three to five separate vendors, each with its own platform, schema, and reporting methodology. The result is data silos that fragment patient journeys, create compliance exposure (consent and audit trails scattered across systems), slow time-to-treatment, and make program ROI impossible to measure consistently. Despite over $5 billion in annual PSP spending, only 3% of eligible patients enroll — and fragmented vendor ecosystems are a direct contributor to that gap. This guide covers the core architecture, the four pillars of PSP operations that fragmentation breaks, and a phased implementation blueprint.
A unified data layer is a centralized integration architecture that consolidates patient, service, and outcome data from all PSP vendors into a single, governed environment. It doesn't replace your vendors; it connects them through standardized APIs, master data management, and a common data model so your team sees one complete picture of every patient's journey.
The fragmentation problem is massive. Despite pharmaceutical companies investing over $5 billion annually in PSPs, only 3% of potentially eligible patients enroll. Data silos contribute directly to this failure: 72% of hospitals report patient data gaps that fragment care journeys, and specialty pharmacy staff struggle because there's no reporting standard between hubs, pharmacies, and manufacturers.
Fragmentation surfaces as four real business problems:
Most PSPs operate across four critical pillars, and fragmentation breaks each one:
Discovery often happens in one vendor’s system while enrollment sits in another. HCPs cannot see if a patient is already engaged, which leads to duplicate outreach, poor experience, and wasted spend. Fragmented data is one of the biggest blockers to accurate patient identification.
Enrollment requires insurance details, prior authorization forms, financial assessments, and consent. When these sit across multiple vendors and channels, teams end up doing manual reconciliation. This slows onboarding, increases compliance risk, and is a major reason only a fraction of eligible patients enroll in PSPs.
Specialty pharma dispensing, cold-chain logistics, nurse visits, and device training must be coordinated as one workflow. With fragmented platforms, no one sees the full handoff. Medication arrives but no nurse is scheduled, or insurance approval is complete but dispatch hasn’t started. These gaps extend time-to-treatment and hurt outcomes.
Refill support, adherence tracking, call-center follow-ups, adverse event reporting, and PV forwarding all require a unified view. Without it safety signals get mixed, adherence definitions vary by vendor, and you cannot prove program performance to payers or regulators.
The compliance risk is acute. Every pillar generates sensitive patient data. When consent and audit trails live across five different systems, audits become slow and risky. A unified PSP data layer gives manufacturers a single, governed source of truth that is audit-ready and defensible.
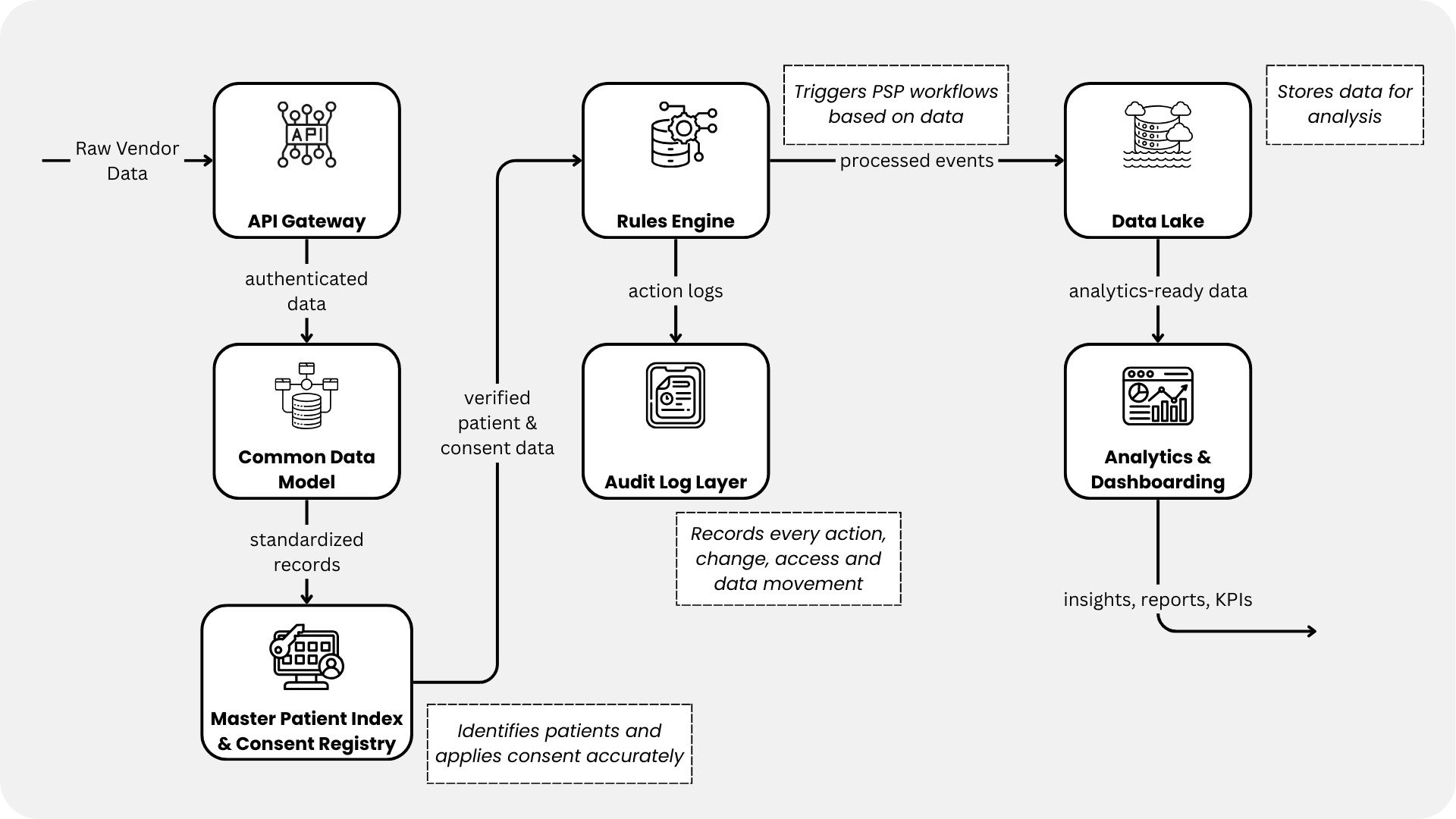
A unified PSP data layer comprises seven core components working together: an API gateway enforcing authentication and enabling real-time data exchange via FHIR and HL7 standards; a common data model mapping disparate vendor schemas to standardized formats; a master patient index with consent registry resolving duplicate records and tracking consent across touchpoints; a rules engine automating workflows like adherence-triggered nurse outreach and payer-specific authorization routing; an audit log layer capturing every data access and modification for FDA 21 CFR Part 11 and GDPR Article 30 compliance; analytics and dashboarding providing unified views of enrollment funnels, adherence trends, and case turnaround; and a data lakehouse storing raw through curated data for both operational reporting and real-world evidence generation.
Most enterprise PSP platforms force you to adapt your workflows to their system design. Rigid SaaS was built for a “best practice” interpretation that doesn’t match your regional compliance rules, internal approval hierarchies, or vendor integrations.
Zelthy’s approach is fundamentally different. As a configurable, open-framework platform built for life sciences, Zelthy adapts to your workflows rather than forcing you to adopt new ones. It digitizes end-to-end PSP processes by aligning with existing SOPs, approval hierarchies, and compliance protocols, ensuring faster adoption, less change management, and a system that feels natural to operational teams.
The distinction matters operationally. When your compliance team needs to add a new regional approval step, they configure it in Zelthy; they don’t wait for a vendor release cycle. When you onboard a new specialty pharmacy vendor with a different data format, Zelthy’s open framework accommodates it without core platform changes. When your program expands to a new therapy or market, the configurable modules apply immediately.
Start with a phased approach that delivers value quickly while managing risk:
Pick the vendor that touches the most patients (specialty pharmacy or hub). Build mappings for enrollment, case status, and adherence events. Validate identity matching and consent enforcement end-to-end. This pilot proves feasibility and surfaces integration challenges before scaling.
Integrate nurse field services, reimbursement hubs, and financial assistance providers. Prioritize vendors that handle the most patient volume or compliance-sensitive data. Implement Master Patient Index to resolve duplicate identities across systems.
Formalize data stewardship roles, audit protocols, and vendor contracts. Ensure consent traceability meets HIPAA minimum necessary standards and GDPR data minimization requirements. Build dashboards for OIG compliance monitoring.
Connect digital PSP tools (apps, telehealth, patient portals) and activate advanced analytics. Deploy predictive models for adherence intervention and real-world evidence collection workflows.
1. Vendor Resistance: Some vendors resist API integration, fearing margin pressure.
Mitigation: Frame integration as mutual benefit—you get data, they get faster case resolution and renewal contracts. Include API development costs in vendor agreements.
2. Duplicate Patient Identities: Different vendors use different identifiers (email vs. phone vs. patient ID).
Mitigation: Implement probabilistic matching algorithms and manual review workflows in your Master Patient Index.
3. Data Latency: Real-time APIs sound great until you discover a vendor's system updates once daily.
Mitigation: Set SLAs in contracts (e.g., case status updates within 4 hours) and build monitoring alerts for delayed data.
4. Consent Mismatches: A patient consents to specialty pharmacy data sharing but not nurse services.
Mitigation: Granular consent management with purpose-specific flags and automated enforcement in your rules engine.
5. KPI Alignment: Vendors define "adherence" differently.
Mitigation: Document standard definitions in your common data model and require vendors to map their calculations to your definitions.
Building or scaling a patient support program?
Zelthy deploys PSP workflows — enrolment, call centre, adherence monitoring — in 4–8 weeks on pre-built templates.
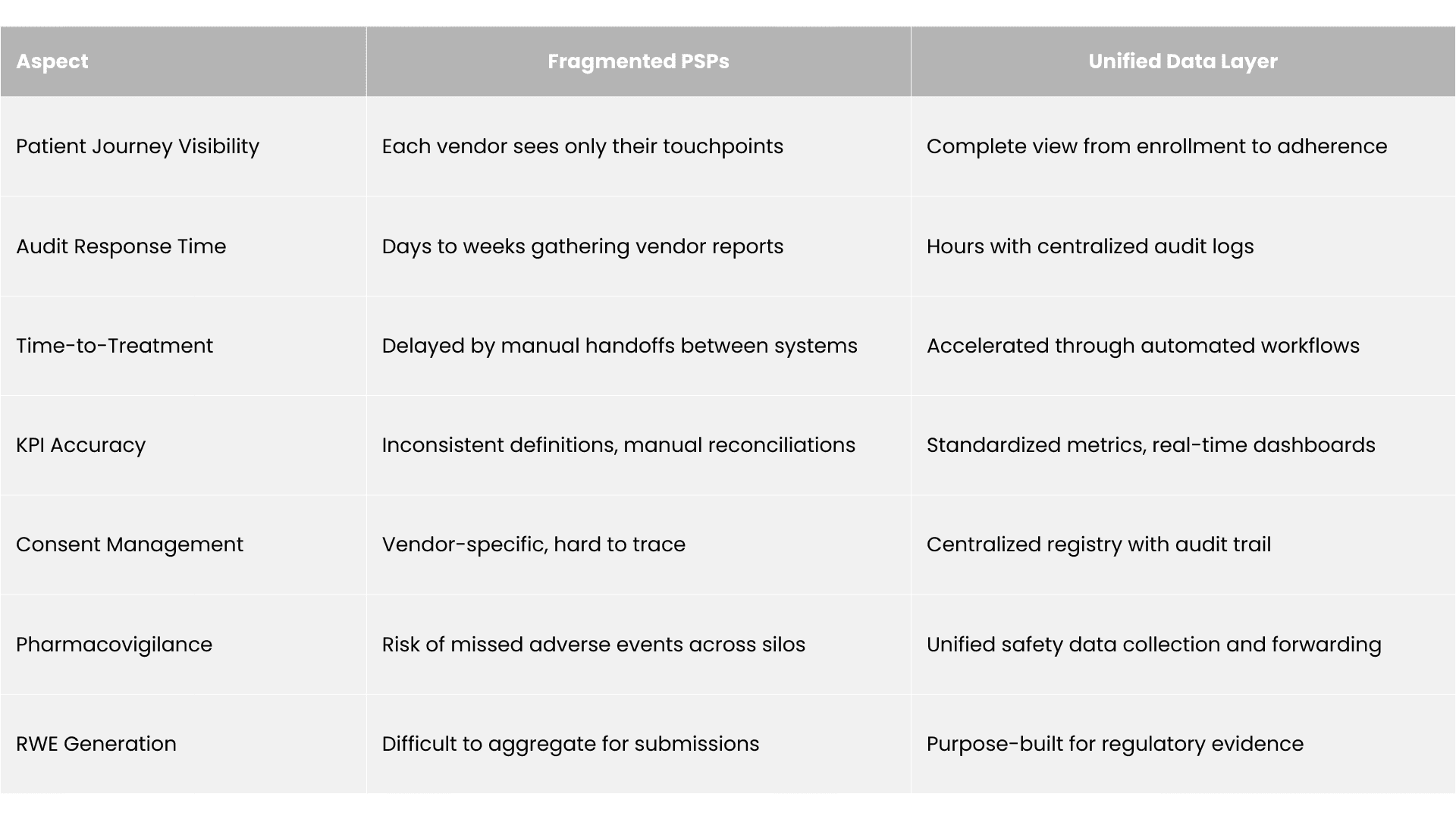
Fragmented PSPs — where each vendor operates its own platform, create slow onboarding (prior authorization and benefits checks hopping between systems), compliance exposure (consent and audit trails scattered across five or more systems), poor patient experience (missed touchpoints, repeated intake, higher dropout), and unreliable commercial reporting (vendors calculating KPIs differently, making program ROI unprovable). A unified data layer resolves each: integrated workflows accelerate prior authorization from weeks to days, centralized consent and audit logs make audits defensible, coordinated touchpoints reduce dropout, and standardized KPIs enable credible payer value demonstrations. Measurable outcomes include 29.3% higher adherence (64.8% vs 50.1%), 28% fewer emergency department visits, 17% fewer inpatient admissions, and 20–40% operational cost reduction.
Reduced Time-to-Treatment: Integrated specialty pharmacy and hub models accelerate prior authorization from weeks to days through uninterrupted data flow and automated compliance checks. A patient moves from “diagnosis flagged” to “treatment started” without manual handoffs.
Higher Patient Adherence: PSPs with unified data show 29.3% higher adherence (64.8% vs 50.1%) and 4.8% months longer median persistence compared to fragmented approaches. When nurses, pharmacies, and call centers see the same patient data and coordinate proactively, adherence improves.
These numbers hold in production. In one deployment, a Zelthy-powered oncology patient support program improved therapy adherence by 45% while cutting operational costs by 30%.
Lower Healthcare Utilization: Unified PSPs reduce emergency department visits by 28% and inpatient admissions by 17% over 36 months. Better adherence and coordinated monitoring catch problems early.
Operational Efficiency: Elimination of manual reconciliations, duplicate data entry, and inter-vendor phone calls cuts operational costs by 20-40%.
Faster Audit Response: When OIG or EMA requests pharmacovigilance data or compliance evidence, a unified system generates reports in hours rather than weeks spent coordinating with five vendors.
Accurate Payer Value Demonstrations: Unified KPIs enable credible real-world evidence submissions to payers, accelerating coverage negotiations and reimbursement decisions.
Zelthy was designed to bring every PSP vendor, workflow, and data stream into one governed ecosystem without forcing teams to rebuild their operations. The platform meets all the requirements of a unified PSP data layer while staying flexible enough to match each organization's real processes.
See the full range of capabilities — from enrollment and adherence monitoring to call centre operations and digital health campaigns, on the Zelthy patient services solution page.
If you want, we can review your current PSP setup and outline what a unified layer would look like. This includes mapping vendor data, defining the consent and identity approach, and identifying where the real ROI will come from. It is often the simplest way to move from abstract conversations about fragmentation to a clear, workable plan that everyone can align behind.
Want to explore how Zelthy can transform your PSP operations? Get in touch with us today. Contact us at connect@zelthy.com or send us a DM on LinkedIn for more information.
A unified PSP data layer is a centralized integration architecture that consolidates patient, service, and outcome data from all PSP vendors into a single governed environment, without replacing those vendors. It connects them through standardized APIs, a common data model, and a master patient index so manufacturers maintain one complete, auditable view of every patient's care journey across hubs, pharmacies, and field services.
When consent records, audit trails, and pharmacovigilance data are distributed across five or more vendor systems, manufacturers cannot produce a unified compliance picture during regulatory audits. FDA 21 CFR Part 11 and GDPR Article 30 both require traceable records of every data access and modification. Fragmented systems make it operationally difficult to demonstrate consent traceability, respond to adverse event queries, or enforce data minimization requirements — turning vendor diversity into a regulatory liability.
A Master Patient Index (MPI) is a database that maintains a single, deduplicated record for each patient across all vendor systems, resolving conflicting identifiers (email, phone, patient ID) used by different hubs and pharmacies. In PSP operations, an MPI links consent status, enrollment history, and care touchpoints to one verified patient record, ensuring that safety reporting is accurate and that patients are not contacted redundantly or omitted from critical follow-ups.
Published data from unified PSP deployments show: 29.3% higher medication adherence (64.8% vs 50.1% in fragmented models), 4.8 months longer median treatment persistence, 28% reduction in emergency department visits, and 17% fewer inpatient admissions over 36 months. Operationally, elimination of manual inter-vendor reconciliation reduces operational costs by 20–40%, while unified KPI reporting enables credible real-world evidence submissions to payers.
GDPR Article 44 restricts transfers of EU patient data to countries without an adequacy decision unless Standard Contractual Clauses (SCCs) or Binding Corporate Rules are in place. A unified PSP data layer must enforce region-specific consent flags, pseudonymize data for cross-border analytics, and apply data residency controls at the architecture level. Consent records must be granular enough to specify per-purpose permissions — for example, differentiating consent for specialty pharmacy from consent for nurse services.
A phased approach manages integration risk while delivering early value. Phase 1 (Weeks 1–8) pilots the highest-volume vendor, typically specialty pharmacy, to validate identity matching and consent enforcement. Phase 2 (Weeks 9–20) expands to hubs, nurse services, and financial assistance providers. Phase 3 (Weeks 21–28) hardens governance, formalizes audit protocols, and ensures HIPAA and GDPR compliance. Phase 4 (Weeks 29–36) activates analytics, predictive adherence models, and real-world evidence workflows.
Rigid SaaS platforms are designed around a fixed interpretation of best-practice PSP workflows, which rarely matches an organization's regional compliance rules, approval hierarchies, and vendor integration requirements. When a compliance team needs to add a new regional approval step or onboard a vendor with a different data format, a rigid SaaS platform requires waiting on vendor release cycles. Configurable platforms that adapt to existing SOPs reduce change management burden and accelerate time-to-value in complex multi-vendor deployments.
Zelthy is pharma's patient services platform — pre-built templates for enrolment, call centre operations, and adherence monitoring, deployed in 4–8 weeks and customised to your therapy and market.
See the Patient Services Solution →![AI Output Compliance Monitoring in Pharma: The Watch Layer [2026]](/_next/image?url=https%3A%2F%2Fhumble-friendship-ab99f71d93.media.strapiapp.com%2FAI_Compliance_in_Pharma_a76c884d28.png&w=3840&q=75)
