
AI Compliance in Pharma: Regulatory Risks, Monitoring Frameworks, and Governance Models
February 11, 2026

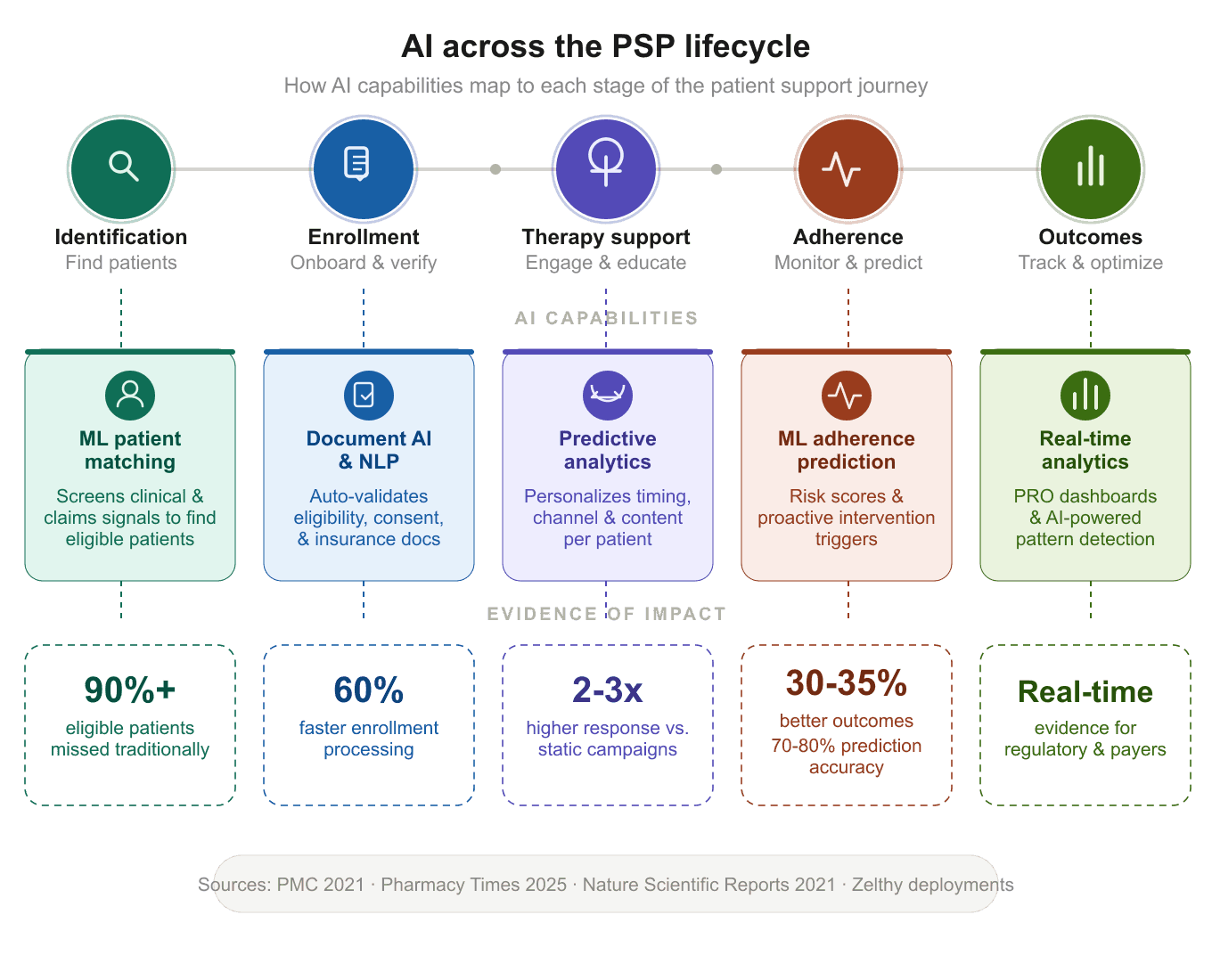
AI in patient support programs refers to the application of machine learning, natural language processing, predictive analytics, and automation technologies across the PSP lifecycle — from patient identification and enrollment through adherence monitoring, adverse event detection, and outcomes reporting. Rather than replacing human coordinators, AI augments program operations by automating structured tasks, surfacing risk signals, and personalizing patient engagement at scale.
Key takeaways from this guide:
AI is transforming patient support programs by automating enrollment validation, predicting therapy drop-off before it happens, detecting adverse events during patient calls in real time, and personalizing engagement across channels. Programs using AI-powered interventions have seen patient outcomes improve by 30–35% compared to standard approaches (PMC, 2021), while platform-based implementations are cutting operational costs by 30–40% and accelerating enrollment by up to 60%.
These aren't incremental improvements layered onto existing call-centre models. They represent a structural shift in how PSPs operate — from reactive, manually intensive workflows to proactive, AI-augmented systems that intervene at the right moment in each patient's journey.
The global PSP market reached an estimated USD 21.8 billion in 2024 and is projected to grow at a 17.1% CAGR through 2034 (InsightAce Analytic). Meanwhile, AI is being embedded directly into the operational layer of these programs, from the hub services that manage patient access to the predictive models that flag adherence risk. In August 2025, Wellgistics Health launched HubRx AI, an AI platform automating core prescription hub functions including eligibility checks and reimbursement support (Grand View Research), illustrating how quickly this integration is accelerating.
Yet the opportunity gap remains enormous. The industry spends billions on patient support programs that most eligible patients never touch. Fragmented vendor ecosystems, disconnected data systems, and one-size-fits-all engagement mean that coordinators spend more time on administrative tasks than on meaningful patient interaction. Legacy hub services platforms and point-solution vendors compound this fragmentation, a challenge that modern PSP platforms are designed to solve. AI addresses each of these failure points, but only when applied systematically across the full PSP lifecycle, not bolted on as a point solution.
This guide maps specific AI capabilities to each stage of the patient support journey, with evidence from peer-reviewed research and production deployments, so that Heads of Patient Services and PSP leads can evaluate where AI will make the biggest operational difference for their programs.
If you're new to the space, start with our complete guide to patient support programs for the foundational framework before diving into the AI layer.
AI in PSPs isn't a single technology, and it isn't a feature bolted onto legacy patient support program software. It's a set of distinct capabilities, each targeting a different operational bottleneck, that work best when deployed on a unified digital PSP platform rather than across disconnected point solutions. The key is understanding which capability applies where in the patient journey.
Enrollment is where the largest volume of eligible patients is lost. Complex eligibility requirements, manual document verification, insurance navigation, and consent management create friction that causes patients to abandon programs before therapy even begins.
AI agents now validate eligibility documents, cross-check insurance coverage against therapy-specific rules, verify consent forms, and flag incomplete applications — reducing the manual bottleneck that historically required dedicated coordinator teams to manage.
Where it applies: Enrollment and onboarding, benefits verification
What it changes operationally: Processing time drops significantly. In platform-based deployments, enrollment has been processed up to 60% faster, with fewer errors and less coordinator time spent on data entry — freeing capacity for the clinical interactions that patients actually need.
Zelthy's patient enrollment and onboarding templates ship with AI verification agents that auto-check eligibility, flag document issues, and route completed applications for approval. The platform supports digital self-service enrollment with document verification, reducing the dependency on phone-based intake processes.
Access barriers — prior authorizations, benefits investigations, co-pay eligibility, are the administrative layer that causes the greatest therapy delays. The pharma hub and patient access support service market alone was valued at USD 3.24 billion in 2024, reflecting the scale of this operational challenge (Grand View Research). Payer-side complexity, including specialty drug formularies and rising claim denials, continues to push manufacturers toward automated solutions.
AI automates benefits investigation, prior authorization tracking, co-pay card eligibility determination, and financial assistance matching. Document processing models extract relevant information from insurance documents and match it against program criteria, reducing days-long manual processes to hours.
Where it applies: Benefits verification, financial assistance, access coordination
What it changes operationally: Patients start therapy faster. In compassionate access programs, AI-augmented workflows have reduced approval times by up to 65%; the difference between a patient waiting weeks and starting therapy within days.
Zelthy's benefits verification and co-pay module automates insurance benefits investigation, prior authorization tracking, and financial assistance workflows. For a real-world example, see how a leading pharma company digitized its compassionate access program, achieving 65% faster approvals and 40% lower operational costs with a 5-week deployment.
For the regulatory framework around compassionate use and expanded access programs, see Expanded Access Basics: When and How Sponsors Should Offer It.
Traditional PSP engagement follows static drip campaigns, pre-defined message sequences sent on fixed schedules regardless of individual patient behavior. These one-size-fits-all approaches produce low response rates and fail to reach patients at the moments that matter most.
AI-driven engagement systems personalize the channel, timing, content, and frequency of communications based on individual behavior patterns. A patient who responds well to SMS reminders at 8 PM receives different engagement than one who prefers email in the morning. A patient approaching a known adherence inflection point (e.g., week 12 of an immunology therapy) gets proactive outreach timed to that milestone.
Where it applies: Ongoing engagement, education, adherence support
What it changes operationally: Higher response rates, better patient satisfaction scores, and critically, engagement resources directed where they have the most therapeutic impact.
Zelthy supports omnichannel engagement across SMS, email, app, and WhatsApp, timed to treatment milestones and individual patient behavior. This is deployed as part of the broader patient education and engagement use case, alongside digital health campaigns and HCP-facing content delivery.
For a detailed breakdown of how therapy management integrates with patient engagement workflows, see our guide to complete therapy management.
Non-adherence remains the most persistent and expensive problem in patient support. The WHO has long estimated that only 50–70% of patients adhere properly to prescribed therapy (Nature, Scientific Reports). In the US, approximately half of the 187 million patients in the healthcare system fail to follow their medication plan as prescribed (Pharmacy Times, 2025).
Machine learning models now analyze refill patterns, patient-reported outcomes, engagement signals, and demographic risk factors to predict which patients are most likely to discontinue therapy, before they actually do. AI has demonstrated 70–80% accuracy in identifying non-adherent individuals for conditions like diabetes and hypertension (Pharmacy Times, 2025). Conversational AI reminder systems have improved adherence rates by more than 20% compared to traditional reminder approaches (PMC, 2023), and an AI clinical data framework achieved 30–35% better patient outcomes compared to treatment-as-usual (PMC, 2021).
Where it applies in the PSP lifecycle: Adherence monitoring, proactive intervention, therapy maintenance
What it changes operationally: Instead of uniform outreach to all enrolled patients, coordinators can focus on the 15–20% at highest drop-off risk. This makes nurse and coordinator time dramatically more productive, shifting from reactive call-back models to proactive, targeted intervention.
Zelthy's medication adherence monitoring module implements this through continuous adherence tracking via refill data, wearables, and PROs, with AI-generated risk scores that surface in coordinator dashboards alongside recommended intervention actions. In production oncology and immunology programs, this has driven measurable adherence improvement and lower operational costs.
For a deeper look at how this fits into a global deployment model, see our analysis of global patient program monitoring platforms.
Pharmacovigilance obligations require that potential adverse events are captured, documented, and reported accurately. In traditional call-centre-based PSPs, AE detection depends on coordinator training and manual post-call documentation, a process that is inconsistent, time-consuming, and prone to gaps.
NLP models now monitor patient conversations in real time, analyzing language patterns that indicate potential adverse events. Flagged events are automatically timestamped, documented with clinical context, and escalated to pharmacovigilance teams, improving both detection rates and regulatory compliance.
Where it applies: Call centre operations, ongoing patient engagement
What it changes operationally: This shifts AE detection from a retrospective, training-dependent process to a systematic, real-time one. Coordinators receive immediate prompts when AE-relevant language is detected, and documentation is auto-generated for compliance workflows.
Zelthy's call centre operations module integrates live AE detection with automatic documentation and escalation pathways. This is particularly critical for oncology and immunology programs where adverse event profiles are complex and reporting timelines are strict.
For the governance and regulatory framework around AI-generated outputs in pharma, see our detailed report on AI compliance monitoring.
Traditional PSP reporting is periodic, manual, and retrospective, quarterly reports assembled from fragmented data sources that show what happened months ago. By the time trends are identified, the window for intervention has often closed.
AI-powered analytics aggregate patient-reported outcomes, adherence data, engagement metrics, and operational KPIs in real time. Pattern detection algorithms identify which interventions are working, which patient segments are underserved, and where program design needs adjustment, enabling continuous optimization rather than annual program reviews.
Where it applies: Outcomes reporting, program management, evidence generation
What it changes operationally: Program managers gain a live view of program health. Regulatory and commercial teams get real-world evidence streams that inform submissions, market access strategies, and program investment decisions.
Zelthy's platform provides real-time outcomes dashboards with AI-powered pattern detection across patient populations, supporting both operational decision-making and the evidence generation requirements that increasingly drive program funding and regulatory submissions.
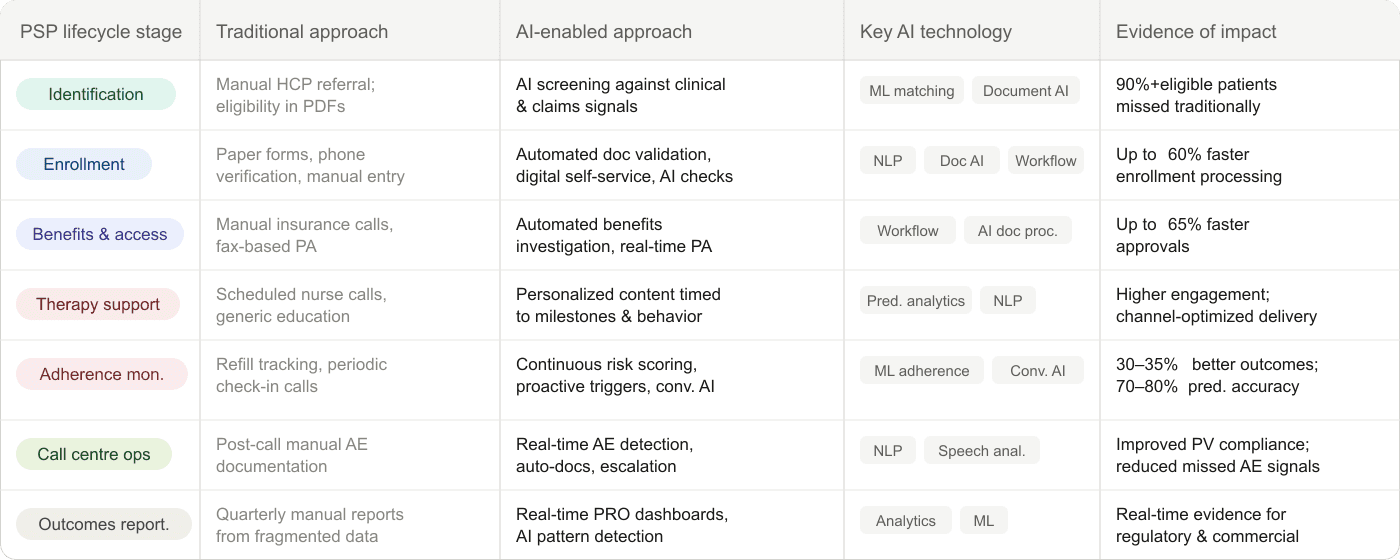
The table below maps each AI capability to the PSP lifecycle stage it impacts, showing the shift from traditional to AI-enabled operations.
A balanced assessment matters here. AI augments the human layer in patient support; it does not replace it.
Clinical judgment. AI surfaces risk scores and recommendations. The decision to intervene, adjust a care plan, or escalate a clinical concern remains with qualified healthcare professionals. No regulatory framework permits fully autonomous AI clinical decisions in patient support settings.
The human connection. Patients dealing with complex therapies — oncology regimens, gene therapy protocols, chronic autoimmune conditions, need human empathy, trust-building, and emotional support. AI's role is to free up coordinator and nurse time so that more of it can be spent on these high-value interactions rather than on administrative tasks.
Regulatory accountability. AI can flag potential adverse events, generate documentation, and track compliance metrics. But regulatory accountability for pharmacovigilance reporting, consent management, and program governance rests with qualified individuals and the sponsoring organization.
Complex case management. Patients with multi-comorbidity profiles, unusual insurance situations, or social determinants that complicate access need human case managers who can navigate ambiguity. AI handles the structured, repeatable work so these professionals can focus on the cases that require human judgment.
The most effective AI-powered PSPs don't automate humans away, they shift the human role from administrative processing to clinical and empathetic engagement. This is the operational model that produces both better outcomes and more sustainable program economics.
Most pharma companies face a three-way choice: build custom AI capabilities in-house, buy point solutions from specialized patient access and adherence vendors, or deploy on an AI-native PSP platform that provides pre-built capabilities with customization flexibility — a modern alternative to legacy platforms like Veeva Vault, IQVIA's patient services stack, or the fragmented hub services model that EVERSANA and Mercalis operate.
Custom builds offer maximum control but typically take 6–12 months and require dedicated data science and engineering teams. Point solutions address individual workflow needs but create vendor fragmentation, a challenge we analyze in detail in unifying multiple PSP vendors under one data layer. Platform approaches deliver pre-built AI agents within weeks while preserving the ability to customize per therapy and market.
AI capabilities in PSPs need data from multiple sources — EHRs, CRMs, pharmacy claims, wearable devices, call centre systems. Integration architecture matters as much as the AI models themselves. Key integration patterns include REST APIs, webhooks, and SFTP support for enterprise systems like Veeva Vault, SAP, Salesforce Health Cloud, and Medidata Rave. Unlike closed-ecosystem vendors that lock data within their platform, an open-architecture approach to PSP software ensures that AI models can access data from any source without proprietary middleware.
AI deployed in patient support must comply with HIPAA, GDPR, and local data protection regulations, plus pharma-specific requirements including GxP compliance, audit trails, role-based access controls, and data sovereignty options. The regulatory landscape for AI in pharma is evolving rapidly; in early 2026, the FDA updated its guidance frameworks in early 2026, specifically revising the Clinical Decision Support (CDS) guidance and the Digital Health Technologies for Drug Development framework, clarifying which AI-enabled tools fall under regulatory scrutiny (Healthcare IT Today, 2026) and which qualify for exemption from device classification. In Europe, the EU AI Act's phased implementation (with high-risk AI system obligations taking effect in August 2026) adds another compliance layer for PSP platforms operating across markets.
For a comprehensive review of the compliance framework, see our guide to AI compliance monitoring in pharma.
Platform-based approaches with pre-built AI agents can move from operational mapping to live patient programs in 4–8 weeks. This includes 1–2 weeks of therapy-specific mapping followed by 4–8 weeks of configuration and deployment, with ongoing optimization. Custom-built solutions typically require 6–12 months.
PSP design and AI implementation vary significantly by market. Regulatory requirements, reimbursement structures, data privacy laws, and patient engagement norms differ between the US, EU, and APAC. Our analysis of patient support program differences between US and EU markets covers these distinctions in detail.
Forward-thinking program sponsors are planning for capability transfer from day one. An AI-native PSP platform that runs on open standards (Python, Django, standard APIs) allows internal teams, including GCC teams, to progressively own and extend the system, rather than remaining permanently dependent on the platform vendor. This is the opposite of the legacy vendor lock-in model, exemplified by per-seat licensing from incumbents like IQVIA and Veeva, that characterizes much of the current PSP technology landscape.
The PSP technology landscape has historically been dominated by three models: large hub services operators (IQVIA, EVERSANA Orchestrate, Mercalis/Valeris), CRM-based platforms extended into patient services (Veeva Vault, Salesforce Health Cloud), and point-solution vendors addressing individual workflow needs (benefits verification, adherence monitoring, call centre operations).
Each has limitations that AI-native platforms are designed to address.
Hub services operators provide end-to-end managed services but create dependency. Program data lives in the operator's systems, customization requires their development teams, and switching costs are high. AI capabilities, when offered, are typically proprietary modules that don't extend to other parts of the program.
CRM-extended platforms offer flexibility but weren't designed for the regulated, patient-facing workflows that PSPs require. Audit trails, GxP compliance, pharmacovigilance integration, and role-based access controls must be custom-built, adding months to deployment and ongoing maintenance burden.
Point-solution vendors address specific bottlenecks well but create the fragmentation problem documented throughout this guide. When enrollment runs on one vendor, adherence on another, and AE detection on a third, the unified patient view that AI needs to generate accurate predictions simply doesn't exist.
An AI-native PSP platform takes a different approach: pre-built AI agents, compliance infrastructure, and workflow templates deployed on a single architecture with open standards. This means:
For pharma teams evaluating PSP technology, the core question isn't whether to adopt AI, it's whether to deploy it within an architecture that compounds its value across the full patient journey or fragment it across disconnected systems.
Zelthy's open-source platform architecture is designed for exactly this use case, providing the AI-native infrastructure that enables the capabilities described throughout this guide.
A global top-10 pharma company needed to replace a manual, paper-based PSP for a flagship oncology therapy that was reaching fewer than 5% of eligible patients. The legacy program relied on fax-based enrollment, manual adherence tracking, and periodic nurse calls with no predictive capability.
Results after AI-powered platform deployment:
Read the full oncology PSP case study →
A leading pharma company's compassionate access program was losing patients in a 12-step manual approval process that averaged 22 days from request to medication dispatch. Every day of delay meant patients with urgent clinical need waited longer for therapy access.
Results after digital transformation:
Read the full compassionate access case study →
Ready to evaluate AI for your patient support program?
See how Zelthy deploys production PSP programs with pre-built AI agents in 4–8 weeks, including enrollment validation, predictive adherence, and AE detection on a single platform.
Request a personalized walkthrough →
This guide isn't written from the outside looking in. Zelthy has deployed over 300 applications across life sciences operations, spanning patient services, clinical trials, commercial operations, traceability, compliance, and regulatory affairs, for pharmaceutical companies including global top-10 organizations operating across 12 countries in Asia-Pacific, the Middle East, and Oceania.
Within patient support specifically, that experience includes production PSP deployments across oncology, immunology, specialty, and rare disease therapies, programs that manage the full lifecycle from patient identification and enrollment through adherence monitoring, call centre operations, and outcomes reporting. The AI capabilities described in this guide — predictive adherence analytics, automated enrollment validation, real-time adverse event detection, are not theoretical. They are running in production programs today, delivering the results documented in the case evidence above.
Three operational patterns have become clear across these deployments:
Most PSP failures are not technology failures; they are fragmentation failures. Programs that run enrollment through one vendor, adherence through another, and reporting through a third create data silos that break the patient journey. AI capabilities compound this problem unless they operate on a unified data layer. This is why Zelthy's platform consolidates all PSP functions and all AI agents on a single architecture rather than bolting AI onto disconnected point solutions.
Deployment speed determines program impact. Every week of implementation delay is a week of patients not enrolled, not monitored, not supported. Zelthy's template-based approach delivers production PSP programs in 4–8 weeks because the AI agents, workflow templates, and compliance infrastructure (audit trails, RBAC, data sovereignty) are pre-built and configurable, not custom-coded from scratch.
Progressive ownership changes the economics. The legacy model, permanent vendor dependency with per-seat licensing, creates misaligned incentives. Zelthy's platform is built on open standards (Python, Django, standard APIs) so that internal teams and GCC organizations can progressively own, extend, and customize the system. The platform is the starting point, not the ceiling.
This operational perspective, built across hundreds of deployments, informs every recommendation in this guide.
How does AI improve patient adherence in support programs?
AI analyzes patterns in refill data, patient-reported outcomes, engagement signals, and demographic risk factors to predict which patients are likely to discontinue therapy. Machine learning models have demonstrated 70–80% accuracy in identifying non-adherent individuals. This enables coordinators to intervene proactively, focusing resources on the patients at highest risk, rather than reacting after a patient has already dropped off. Programs using AI-powered interventions have seen outcomes improve by 30–35% compared to standard care approaches.
What types of AI are used in patient support programs?
The main AI technologies in PSPs include: machine learning for adherence prediction and patient risk scoring; natural language processing (NLP) for real-time adverse event detection during patient calls; document AI for automated enrollment validation and benefits verification; predictive analytics for personalized engagement timing and channel optimization; and conversational AI for medication reminders and patient communication. Each targets a different operational bottleneck in the PSP lifecycle.
How long does it take to deploy AI in a patient support program?
Platform-based approaches with pre-built AI agents can go live in 4–8 weeks, including operational mapping (1–2 weeks) and configuration and deployment (4–8 weeks). Custom-built solutions typically require 6–12 months. The key variable is integration complexity; programs that need connections to multiple enterprise systems (EHR, CRM, claims data) require more configuration time.
Is AI in patient support programs compliant with healthcare regulations?
AI in PSPs must comply with HIPAA, GDPR, and local data protection regulations, plus pharma-specific requirements like GxP, pharmacovigilance reporting obligations, and audit trail requirements. Compliant implementations require role-based access controls, data sovereignty options, and human oversight for clinical and regulatory decisions. The FDA updated its guidance frameworks in early 2026, clarifying the regulatory treatment of AI-enabled clinical decision support tools.
Can AI replace nurse coordinators in patient support programs?
No. AI augments coordinators by automating administrative tasks — enrollment validation, documentation, scheduling, adherence tracking, and surfacing actionable insights like risk scores and intervention recommendations. This frees coordinators to spend more time on clinical judgment, emotional support, and complex case management, the interactions that require human expertise and that patients value most.
What is the ROI of AI in patient support programs?
Measurable ROI includes faster enrollment (reducing time-to-therapy), higher adherence rates (improving therapy outcomes and commercial performance), lower operational costs (30–40% reduction through automation), and improved pharmacovigilance compliance. Programs also generate richer real-world evidence streams for regulatory submissions and commercial strategy. The global digital medication adherence market alone is projected to reach USD 6.8 billion by 2026.
How do AI-native PSP platforms differ from legacy hub services providers?
Legacy hub services providers (such as large managed service operators) typically run patient support as an outsourced service with proprietary technology, creating vendor dependency and data silos. CRM-based platforms extended into patient services often lack built-in compliance infrastructure for regulated pharma workflows. AI-native PSP platforms take a different approach: pre-built AI agents, GxP-ready compliance infrastructure, and workflow templates deployed on a single open-source architecture. This means AI models operate on unified patient data rather than fragmented vendor systems, internal teams can progressively own and extend the platform, and production programs can deploy in weeks rather than months.
How does AI handle adverse event detection in patient calls?
NLP models analyze patient language during live calls, identifying phrases and patterns that indicate potential adverse events. Flagged events are automatically documented with timestamps and clinical context, escalated to pharmacovigilance teams, and integrated into compliance reporting workflows. This reduces the risk of missed AE signals, a persistent challenge in traditional call-centre-based PSPs where detection depends on individual coordinator training.
What data does AI need to work effectively in a PSP?
AI models in PSPs typically use enrollment data, pharmacy refill records, patient-reported outcomes, engagement interaction data (call logs, message responses), claims data, and where available — wearable device outputs. The more data sources integrated, the more accurate predictions become. However, even starting with refill and engagement data alone provides meaningful adherence risk signals that improve coordinator efficiency.
AI in patient support is moving from pilot to production. The convergence of AI capabilities, platform-based deployment models, and increasing regulatory clarity means that the operational barriers to adoption are lower than ever, while the cost of inaction grows as competitors digitize.
For pharma teams evaluating their options: the decision is less about whether to adopt AI in PSPs and more about which capabilities to deploy first and on what architecture.
Zelthy's AI-powered patient services platform ships with pre-built AI agents for enrollment validation, adherence prediction, AE detection, and compliance monitoring, deployed in 4–8 weeks on an open-source framework with full code ownership.
Want to see this in action for your therapy area? Request a personalized walkthrough →
For further inquiries, reach us at connect@zelthy.com or send us a message on LinkedIn.

